

ADPKD is a genetic disease and the fourth leading cause of ESKD4,5
ADPKD is characterized primarily by the development and progressive enlargement of fluid-filled renal cysts.6
- Cysts enlarge the kidneys and impair their ability to function normally, and can lead to debilitating consequences such as ESKD, dialysis, or kidney transplantation7
- The rate of progression in ADPKD can vary from patient to patient4,8
- Patients identified as being at high risk of rapid disease progression are likely to reach ESKD at an earlier age than expected10

KNOW THEIR PROGRESSION
Assessing the rate of progression is an important step in the management of ADPKD to delay further kidney damage1,11
ESKD=end-stage kidney disease.
Consider a proactive approach to assessing disease progression
Don’t wait for kidney function decline1
Determining ADPKD disease progression requires more than monitoring kidney function alone1
- Patients with ADPKD may remain asymptomatic for years while the disease progresses, likely due to compensatory hyperfiltration1,12
- ADPKD can progress significantly while eGFR presents as normal or is slightly decreased. A normal eGFR may be masking irreversible kidney damage1,2
- Patients exhibiting a rapid decline in eGFR are already in a state of rapid disease progression10*
Rapid disease progression may be identified by a confirmed eGFR decline ≥5 mL/min/1.73 m2 within 1 year or by an average annual eGFR decline
of ≥2.5 mL/min/1.73 m2 over a period of 5 years.


(total kidney volume)
- Healthy nephrons compensate for damaged nephrons in the early stages of ADPKD. This causes eGFR to appear normal or only slightly reduced, despite the fact that damage is occurring2,13
- While eGFR remains stable, kidney volume is 4 to 6 times greater than normal, and the kidney is irreversibly damaged14
- As much as half of the renal parenchyma can be lost with no real derangement in renal function15
ACT NOW, BEFORE IT’S TOO LATE…
ADPKD can progress significantly even with a stable eGFR. Determine your ADPKD patients’ rate of progression by looking at factors other than eGFR.1,13

(total kidney volume)
- Progression of ADPKD can often go unnoticed. Normal kidney function can mask the severity of disease progression until irreversible damage has already occurred1
- In most patients with ADPKD, eGFR levels do not decline until they are 40 or 50 years old, when kidneys are grossly enlarged8
SEE MORE THAN eGFR
Total kidney volume can help assess the rate of progression and predict future decline of kidney function3
According to the US Consortium for Radiologic Imaging Studies in Polycystic Kidney Disease (CRISP) cohort analysis published in Kidney International:
A one-time kidney size measurement can assess the rate of progression and predict the future decline of kidney function3
- CRISP has shown that kidney enlargement is an early manifestation of ADPKD3
- Prognostic tools such as the TKV-based Classification of ADPKD may help identify the rate of rapid disease progression before rapid decline of kidney function occurs17
Know your patients’ kidney size
In ADPKD, kidney growth and damage often occur before kidney function declines. Kidney size is the best predictor of the rate of ADPKD progression.
The Consortium for Radiologic Imaging Studies of Polycystic Kidney Disease (CRISP) is a National Institutes of Health-funded, 14-year observational study (N=241) of adult ADPKD patients. The primary goal was to determine the extent to which TKV forecasts the development of renal insufficiency in ADPKD.
TKV=total kidney volume.
Section with opacity
Imaging your patients’ kidneys can help predict their risk of disease progression in ADPKD17,18
There are multiple ways to measure kidney size


Kidney Volume
MRI or CT scan can reliably measure kidney size to calculate TKV17,18,†
- Identifying a TKV greater than expected for patient’s age can provide an early and reliable marker for rapid disease progression and predict future kidney function decline19,20
- Determine ADPKD Imaging Classification using the Mayo Imaging Classification tool to assess if patient may be at risk of rapid progression18

Kidney Length
In younger patients, ultrasound kidney length can be used when MRI/CT-calculated TKV is not available10,18
- Based on the CRISP study, ultrasound kidney length >16.5 cm in patients aged <45 years can indicate a risk of rapid progression10,18
- In the CRISP study, a kidney length of
>16.5 cm was shown to predict development of CKD Stage 3 within 8 years in patients with ADPKD who were <45 years of age and who had CKD Stage 1 or 221,§
- In the CRISP study, a kidney length of
- Ultrasound can be used to determine TKV, but may not be as reliable as MRI/CT due to inter- and intraoperator variability.
- Average baseline GFR of 98 mL/min/1.73 m2.
Learn how to measure TKV
TKV measurement techniques18,19
Manual Segmentation:
Request TKV from radiologist
Ellipsoid Formula:
- Request measurements: kidney length, width, and depth
- Calculate TKV using the ellipsoid formula
π/6 • (L x W x D) = TKV (mL) - Calculate htTKV using the patient’s height and TKV
TKV/height (m) = htTKV (mL/m)
htTKV=height-adjusted total kidney volume.
The Mayo Imaging Classification can help
assess the rate of progression
using htTKV and age18,¶
Patients in Classes 1C, 1D, or 1E are at high risk for rapid progression
Patients in Class 1B are at intermediate risk for eGFR decline and could be re-evaluated at yearly intervals to determine risk for progression
Patients in Class 1A are at low risk for eGFR decline
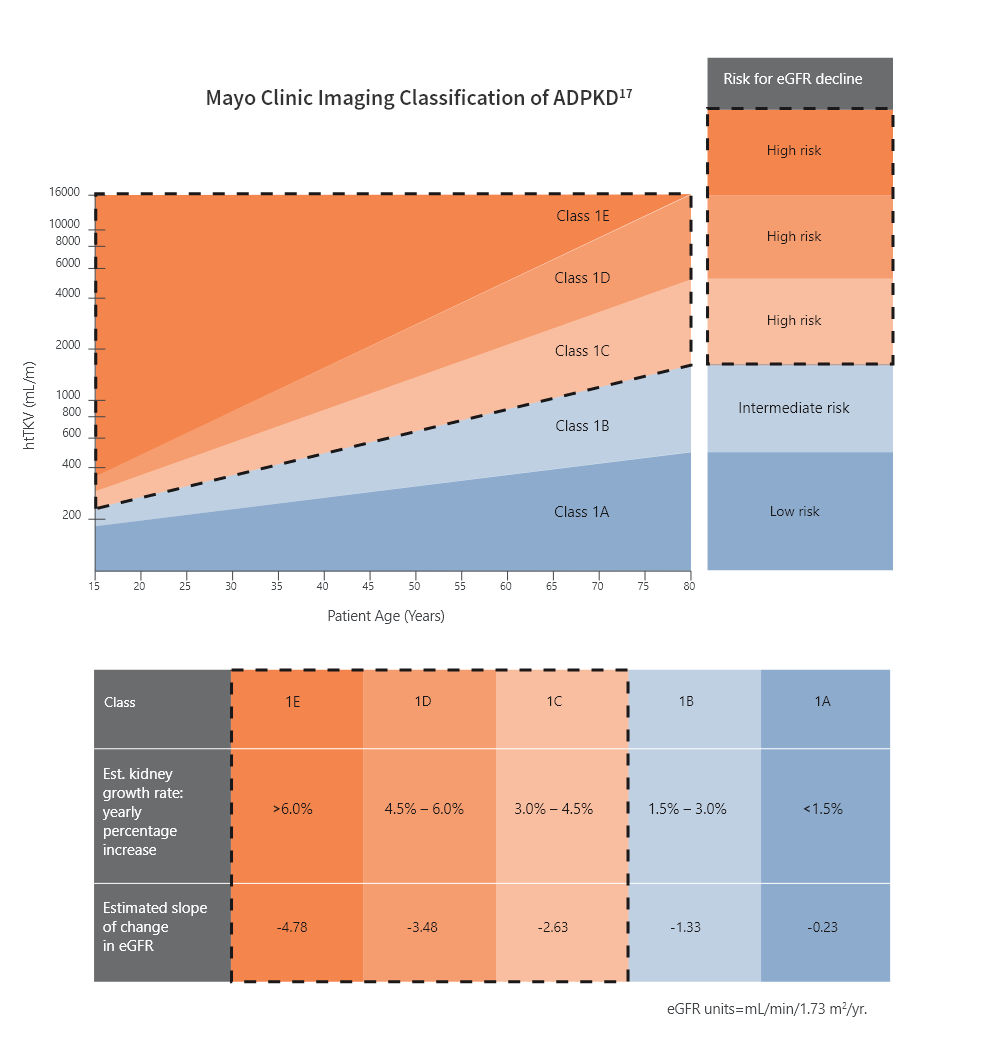
Republished and adapted with permission of the American Society of Nephrology, from Imaging classification of autosomal polycystic kidney disease: a simple model for selecting patients for clinical trials. J Am Soc Nephrol. 2015;26(1):160-172.
Bilateral and diffuse distribution, with mild, moderate, or severe replacement of kidney tissue by cysts, where all cysts contribute similarly to TKV. Classification applies only to patients with typical morphology of ADPKD as defined by diffuse bilateral cystic involvement of the kidneys.17
CKD=chronic kidney disease; CT=computed tomography; htTKV=height-adjusted total kidney volume; KDIGO=Kidney Disease: Improving Global Outcomes;
MRI=magnetic resonance imaging.
Section with opacity
Section with opacity
Once you have assessed your patient's kidney size, learn more about a treatment option for ADPKD
KDIGO Guidelines recommend referring your patients who have hereditary kidney disease, like ADPKD, to a nephrologist.
If you are a primary care physician and want to better understand disease progression and treatment options, consult with a nephrologist.
References
1. Grantham JJ, Chapman AB, Torres VE. Clin J Am Soc Nephrol. 2006;1(1):148-157. 2. Grantham JJ, Mulamalla S, Swenson-Fields KI. Nat Rev Nephrol. 2011;7(10):556-566. 3. Yu ASL, Shen C, Landsittel DP, et al; for the Consortium for Radiologic Imaging Studies of Polycystic Kidney Disease (CRISP). Kidney Int. 2019;95(5):1253-1261. 4. Helal I, Reed B, Schrier RW. Am J Nephrol. 2012;36(2):162-167. 5. Schrier RW. J Am Soc Nephrol. 2010;21(6):861-863. 6. Patel V, Chowdhury R, lgarashi P. Curr Opin Nephrol Hypertens. 2009;18(2):99-106. 7. Harris PC, Torres VE. Annu Rev Med. 2009;60:321-337. 8. Grantham JJ, Torres VE, Chapman AB, et al. N Engl J Med. 2006;354(20):2122-2130. 9. Chebib FT, Torres VE. Am J Kidney Dis. 2016;67(5):792-810. 10. Gansevoort RT, Arici M, Benzing T, et al. Nephrol Dial Transplant. 2016;31(3):337-348. 11. Grantham JJ, Torres VE. Nat Rev Nephrol. 2016;12(11):667-677. 12. Ness B, Stovall K. JAAPA. 2016;29(12):24-28. 13. Grantham JJ. N Engl J Med. 2008;359(14):1477-1485. 14. Braun W. Cleve Clin J Med. 2009;76(2):97-104. 15. Gaur P, Gedroyc W, Hill P. Br J Radiol. 2019;92(1098):20190078. 16. Chapman AB, Wei W. Semin Nephrol. 2011;31(3):237-244. 17. Irazabal MV, Rangel LJ, Bergstralh EJ, et al. J Am Soc Nephrol. 2015;26(1):160-172. 18. Magistroni R, Corsi C, Martí T, Torra R. Am J Nephrol. 2018;48(1):67-78. 19. Chapman AB, Bost JE, Torres VE, et al. Clin J Am Soc Nephrol. 2012;7(3):479-486. 20. Yu ASL, Shen C, Landsittel DP, et al; for the Consortium for Radiologic Imaging Studies of Polycystic Disease (CRISP). Kidney Int. 2018;93(3):691-699. 21. Bhutani H, Smith V, Rahbari-Oskoui F, et al. Kidney Int. 2015;88(1):146-151.